SKIN INFECTIONS: IMPÉTIGO. Clinical case in a 3 year old girl.
Best regards to the entire Steemit community, especially to the members and readers of the scientific community, in this publication I wanted to share with you about this pathological entity, which constitutes a skin infection caused by bacteria, that often affects more severely the pediatric patient, and something that brows my attention it's the fact that the frequency of this infection in our current environment has gone really high, as a result of the neglect of the responsible adult; as well as the scarce information about the basic hygienic measures that would serve as preventive barriers.
Therefore, always thinking of contributing a grain of sand by sharing a little of the knowledge that I've had obtain during my internships at the hospital during my training, I prepared this publication, with some information about this disease and the presentation of a clinical case that came to the Pediatric Emergency during one of my turns in that service.

Before beginning to explain about this pathology, it's important to make a brief review on the histology of the skin, in order to have a better understanding of how it can be affected by various microorganisms, at different levels:
The skin forms the outer wall of the body, being the barrier that defends us from different alterations, and is constituted by 2 layers:
Epidermis: It's the most superficial layer, formed by a stratified epithelium of several cell layers that evolve from depth to surface. As a general rule, infections limited to this area are considered low risk or uncomplicated.
Dermis: It's the middle and most voluminous layer of the skin, and is in turn formed by two cell layers: the papillary and the reticular layer. The dermis integrates with the subcutaneous tissue, without having a well defined boundary between the two (for this reason, in many bibliographies the ST is taken into account as a third layer of the skin).
Infections that affect various degrees of the dermis and / or subcutaneous tissue will be considered as low or high risk in relation to the depth they reach, and the probability of developing systemic complications or not.
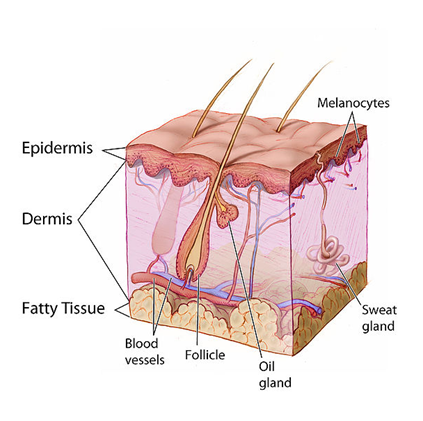
Source: Wikipedia. Anatomy of the skin
Based on this, we can see that infections that affect the skin may be limited to the most superficial layer of the skin, or they may deepen and reach deeper layers, greatly complicating the clinical situation, and expanding the type of treatment that will be needed.
Within the wide range of skin infections that can occur, the microorganisms that cause them are usually the two main ones: Staphylococcus aureus and Streptococcus pyogenes. Therefore, the treatment has as a general rule, the use of antibiotics that cover both bacteria, and this usually it's indicated once the diagnosis has been installed.
Said diagnosis is clinical, in the vast majority of cases, based on both the patient's history and a exhaustive physical exam.
Therefore, in skin infections caused by bacteria, those whose etiology is staphylococcus and streptococcus, are one of the most frequent dermatological diagnoses, being Impetigo, the clinical form of greatest presentation in pediatric age.
WHAT IS IMPETIGO?
It's a superficial skin infection limited to the epidermis, very common in children, with a peak of maximum incidence between 2 and 6 years old, and it's related to factors of inadequate personal hygiene and overcrowding, since it's highly contagious, and spreads mainly through direct contact.
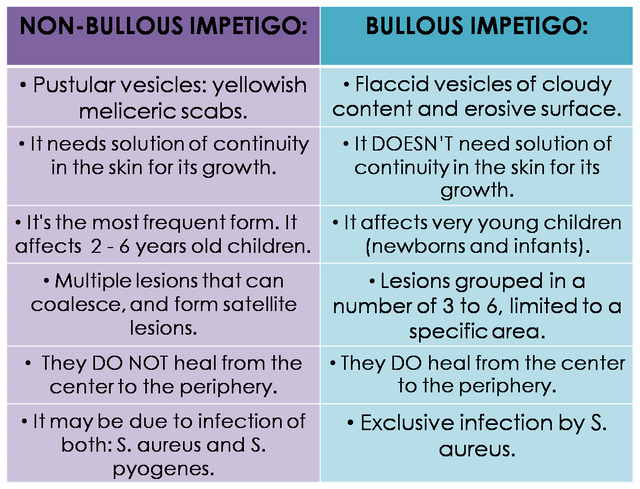
It's caused by S. aureus, S. pyogenes, or both. Clinically it's not easy to differentiate between impetigo caused by one or another microorganism, however there are typically two clinical forms of presentation of this pathology, among which we can observe a series of differences.
- Non-Bullous Impetigo: It's also called microvesiculous, because of the appearance of the lesions, or contagious, because it's the fastest-spreading clinical form. With up to 70% of cases, it constitutes the most frequent form of impetigo. It's characterized by requiring a solution of continuity in the skin for its appearance, since it usually begins in areas of trauma (superficial wounds, insect bites, wounds or varicella scars). The lesions are typically vesicle-pustules that break easily, leaving yellowish crusts in their path.
These lesions are multiple, and can sometimes coalesce, they spread by self-inoculation so satellite lesions can form.


{kind=link}
- Bullous Impetigo: It's less frequent than the previous form, and is always caused by S. aureus, by the action of its toxins. It's characterized by flaccid vesiculous lesions of cloudy content and erosive surface, which appear grouped in groups of 3-6 and remain limited to one area, being the most frequent areas of greatest exposure such as face, and extremities. It represents the localized form of staphylococcal scalded skin syndrome.
HOW TO DIAGNOSE IT?
The diagnosis of Impetigo is based on the clinical aspect of the lesions: Meliceric crusts or flaccid blisters with erosive surface.
And later it will be confirmed with the performance of the Gram test, and cell culture of the liquid content or the surface of the lesions.
WHAT IS ITS TREATMENT?
It's based on the symptomatic treatment of the disease, as well as the prevention of its dissemination:
- Good personal hygiene (it's important to trim the child's nails, to prevent the spread of self-inoculation injuries).
- Topical antimicrobial treatment:
- Fusidic acid or Mupirocin (2-3 times a day for 10 days).
This constitutes the first choice treatment for localized forms of the disease, and limits the spread of the disease.
- Systemic antibiotic: It will only be necessary under certain circumstances, such as: multiple / large-scale injuries / difficult-to-treat locations, underlying factors of the patient, in case it affects several family members and / or school. Effective antibiotics should be used against both microorganisms that cause impetigo, such as: Cefadroxil, Amoxicillin + Ac. Clavulanic, Penicillin or Amoxicillin, Cloxacillin, or Macrolides in case of allergy to beta-lactams. The use of systemic antibiotics produces faster healing, and prevents the spread of the disease to deeper layers of the skin.

Reason for consultation: Multiple skin lesions.
Current Disease: This is a 3-year-old female preschool, natural from the locality, who is brought by her mother when presenting the clinical of 4 days of evolution, characterized by the presence of multiple lesions vesiculo-bullous cutaneous, which began its appearance from a superficial lesion located in the lower left limb in the malleolar region, subsequently spreading rapidly until being located in both lower limbs, thighs, perineum, abdomen, and both upper limbs. Which were accompanied by pruritus and malaise. Reason for which prior medical evaluation is decided to enter the pediatric observation area of the hospital.
Background of Importance:
Dietary transgressions from 2 months old: Exclusive breastfeeding for 2 months, with premature onset of ablactation.
Incomplete undocumented immunization schedule.
Hospitalization at 8 months old, due to pneumonia acquired in the community for 7 days.
Socio-economic situation: Family members report current overcrowding in the home where the girl lives. As well as unemployment situation of both parents.
Physical exam:
- Vital Signs:
Blood pressure: 122/71 mmHg / Heart rate: 88 x' / Breathing frequency: 22 x' / Temperature°: 36.8 °C.
Patient in stable clinical conditions, hydrated, eupneic, afebrile to the touch, with adequate cutaneous-mucosal coloration.
Normocephalic, well implanted hair, normo light reactive isocoric pupils, well implanted atrial pavilion, nasal and oropharyngeal mucosa without alterations. Adenomegaly is not palpated in the neck. Symmetric thorax, conserved expandability, audible lung noises in both lung fields, without aggregates. Rhythmic heart sounds without murmurs. Abdomen soft, depressible, not painful to superficial and deep palpation, without visceromegalies.




Diagnosis:
It was performed in a clinical way. Therefore, no additional tests were requested.
(In part because of the socio-economic situation of the parents, who did not have the monetary means to carry out the exams, and they were not available for free in the institution).
Management:
The lesions were cleaned with physiological solution and hydrogen peroxide in the pediatric observation area, in the presence of the parents so that they observed how to do it at home. During the cleaning some of the lesions were broken, releasing a clear non-purulent liquid. Subsequently Fusidic Acid was applied in cream, in all the lesions, which were left without cover.
Among the recommendations we made to parents were:
- Improve the personal hygiene of all family members.
- Trim the girl's nails, and monitor / avoid continuous scratching of the lesions.
- Application of Fusidic Acid in cream 3 times a day, for 10 consecutive days.
- Be alert to the appearance of a greater number of lesions, their progression, response to treatment, or the appearance of systemic symptoms such as fever. As well as the appearance of similar lesions in another family member.
- Go to the hospital before any of the situations mentioned above.
• CONCLUSIONS:
[1] Bacterial skin infections. E. Sellarés Casas, F.A. Moraga Llop.
[2] Arthur Rook; D.S. Wilkinson; F.J.G. Ebling Dermatology Treaty. Fourth edition.
[3] Infectious Diseases Committee. Red Book 2003. American Academy of Pediatrics.
[4] Fonseca Capdevila, Eduardo. Pediatric Dermatology 1st edition 2001.
[5] Ralph Feigin; James D. Cherry Treaty of Infectious Diseases in Pediatrics. Third edition.

@tipu curate
Upvoted 👌 (Mana: 0/20 - need recharge?)
Hello I always read your articles very willingly, and our community very much appreciates this type of work, well done!
riccc96
Hello,
Your post has been manually curated by a @stem.curate curator.
We are dedicated to supporting great content, like yours on the STEMGeeks tribe.
If you like what we are doing, please show your support as well by following our Steem Auto curation trail.
Please join us on discord.
To listen to the audio version of this article click on the play image.

Brought to you by @tts. If you find it useful please consider upvoting this reply.