Ovarian tumor. Clinical case.
Ovarian tumors are common findings in gynecology in general. Out of these, most of them correspond to benign neoplasms fortunately. In this article, the most important points in relation to the subject will be discussed as a summary, for the subsequent presentation of a clinical case of this pathology.
Among the most important and necessary aspects for the understanding of the subject, the classification of these neoplasms stands out, since there is a large number of forms of presentation, between benign and malignant forms; Likewise, the most important characteristics regarding the diagnosis and treatment of this disease will be briefly explained.

Ovarian tumors can originate from the epithelium, germ cells, or stroma of the sex cords, thus distinguishing histologically. Similarly, the ovary can be a site for the growth of metastatic tumors, coming from neighboring or distant anatomical structures that gave rise to it in the first place.
In this way we can find the following types of tumors at the ovarian level:
• Superficial, Celomic or Germinative Epithelial Tumor: They constitute more than 70% of all ovarian tumors, being by far the most frequent of all. And depending on their nature, they will be called Carcinoma (when they are Malignant), and Cystadenomas (those Benign).
• Germ Cell Tumors themselves: cover about 20% of ovarian neoplasms. This includes Teratomas, Endodermal Sinus Tumors, Choriocarcinomas and Dysgerminomas as the most frequent.
• Ovarian Stroma Tumors (of the sexual cords): they are constituted by fusocellular cells that have a great power of differentiation (they are the Teak cells). These tumors are hormone producers, and represent 10% of all ovarian neoplasms. They are: granulose tumors, fibroids, fibrotecomas, tecomas, tumors of Sartoli and Leydig cells.
• Metastatic Tumors: These are tumors of origin that are either near or distal to the ovary, but that have settled at this level thanks to the metastatic process, which can occur either via continuity, blood or lymph; the main tumor that metastasizes at the level of the ovary originates in the digestive tract, and manifests as large clusters of * seal ring cells *, receiving the name of Krukenberg tumor; These are highly aggressive malignancies due to their metastatic nature, which indicates that they have already exceeded the limits of the organ affected by the primary tumor.
The following image shows a more schematized classification, where the most frequent tumors within each group of neoplasms are mentioned:

Regarding the epidemiology and pathogenesis of the disease, we see that although it's mostly benign forms, ovarian tumors represent 6% of all malignant neoplasms in women, and around the 8th cause of death. It's responsible for 50% of deaths from malignant neoplasms originating in the genital tract (only surpassed by the pathology of the cervix and endometrium).
The risk factors are not very well established, but they have been highlighted: nulliparity (on the contrary, multiparity is considered a protective factor), family history (first-degree relatives with ovarian cancer increases up to 3 times the risk of suffering such pathology ), and genetic factors (the presence of certain proto-oncogenes has been related to the development of any of these tumor forms).
Clinical Aspects:
The diagnosis is usually carried out in advanced stages of the disease; The main clinical manifestation by which the patients go to the doctor is to present an increase in the abdominal perimeter or ascites (this means that the tumor has already metastasized in the peritoneal cavity: Peritoneal Carcinomatosis; therefore it's sign of bad prognosis). Other clinical manifestations include abdominal or pelvic pain and increased regional volume. In addition to this, all ovarian tumors of a malignant nature have the general manifestations of any type of neoplasm, such as: malaise, weight loss, asthenia, etc. But the most important thing is the presence of ascites, since there's an intimate relationship between the ovary and the peritoneal cavity, and especially the tumors of the epithelial line tend to exceed the limits of the organ in very early stages of the disease.
However, it's well known that this pathology can occur in a significant number of patients, asymptomatically; reason why the diagnosis is usually carried out already in very advanced stages as mentioned above.
Then the following question arises:
How is the diagnosis of an Ovarian Neoplasm made?
All the diagnostic elements we know should be taken into account:
Clinical History thorough: An adequate history should be carried out that allows us to inquire about the risk factors that may be present in each patient, whether personal or related to their immediate family members.
Physical Exam: The clinical conditions of the patient should be evaluated, with special emphasis on signs that suggest the presence of chronic and / or malignant disease: marked pallor, weight loss, tired facie, etc. Similarly to the abdominal clinical examination, through the bimanual palpation the possible existence of adnexal masses and their characteristics, as well as ascites (accumulation of fluid in the abdominal cavity) will be investigated.
Images: The best technique is Ultrasound, either Pelvic-Transvaginal (TVS) or Abdominal (TAS); since most ovarian tumors have a cystic component, which can be observed very well through ultrasound. The size of the neoplasm constitutes the main factor to choose which one between both (TVS or TAS).
- Tumor Markers: These substances are proteins produced by the cells of a tumor or by the organism in response to the tumor cells. Many of these markers have been used for the identification of ovarian cancers; However, they are not always so specific.
Some of the most used are:
- CA125 and CA19-9: they rise in many cases of ovarian carcinomas, that is, neoplasms originating from the superficial or celomic epithelium.
- Alpha fetoprotein: it is elevated in cases of neoplasms originating from germ cells, for example Tumor of the Endodermal Sinus.
- Beta-HCG (Human Chorionic Gonadotrophin): usually occurs at very high levels in cases of Choriocarcinomas.
These markers not only have a diagnostic value, but also serve as a way to assess the prognosis, since it allows us to monitor each patient's treatment, informing about the evolution of the disease and the type of response.
Treatment:
In spite of the continuous advances in medicine in relation to the diagnostic methods of this type of pathologies, even today it's very difficult from the clinical point of view, to differentiate between an ovarian neoplasm of a benign or malignant nature. For this reason in the treatment it is necessary to balance the concern for performing a surgical intervention because of a benign lesion, with the risk of not removing an ovarian cancer.
However, most ovarian neoplasms are made up of tumors of epithelial origin, where the most common are those of a cystic nature; within this group we see how most ovarian cysts are functional, and almost all suffer spontaneous regression in the next six months of their detection, so expectant behavior is the most recommended. For this, certain criteria have been established, which must be met so that this type of treatment is the most indicated:
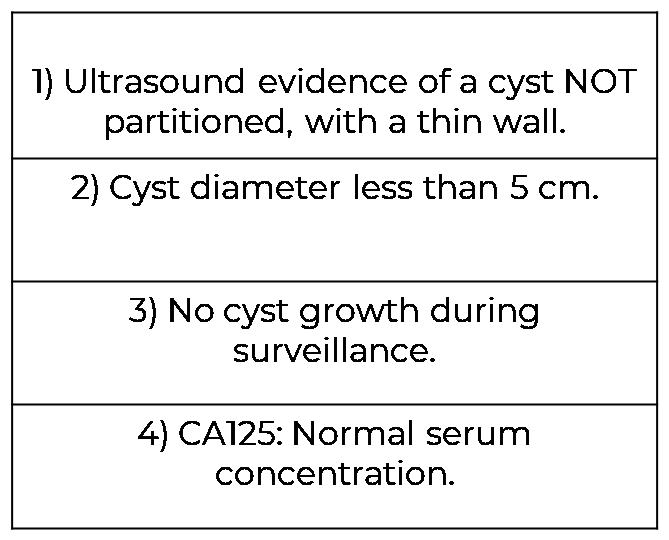
Image Source: Own elaboration chart with the use of the Microsoft Power Point program.
While in those tumors that don't meet the aforementioned characteristics, the definitive therapeutic tool is the surgical ablation of the tumor (as previously explained, the morphological similarity between the various cysts, even between malignant and benign).
And the decision to resort to one technique or another will depend on the size of the lesion, the age of the patient, and trans-surgical findings.
Here we must remember the importance of the individualization of each case, for example, in a premenopausal woman, it's enough to ablate the cyst before a small lesion, preserving reproductive function. In case of a larger lesion, an oophorectomy should be performed because of the difficulty in enucleating the cyst without breaking it and the increased risk of cancer in these large cysts. However, in a postmenopausal woman it is preferred to resort to oophorectomy regardless of the size of the lesion, since the risk of cancer is high in this age group, and the benefits offered by preserving the ovary are minimal.
The patient was Rosa Hernández, 59 years old, with the following important pathological antecedents: Chronic controlled arterial hypertension, Bilateral nephritis with chronic renal damage that required renal transplantation 15 years ago, and Diabetes Mellitus due to prolonged use of steroidal medications .
Mrs. Rosa consulted with her internist doctor on a routine visit, about something that had plagued her for some time, but she had not yet felt the need to tell her, for believing that it was * "ailments of age" *, she was presenting a progressive * increase in the volume at the abdominal level *, it didn't hurt, nor did prevent her from any activity, so it didn't concerned her until it didn't obtain a significant size.
Her internist doctor performed a thorough physical examination, through which he couldn't deduce the cause of the increase in the abdominal perimeter in the patient; and after performing a series of tests, which included an abdominal ultrasound, the presence of a cystic mass at the level of the right ovary of a considerable size could be detected; This is why the patient was referred to a specialist in the area of Gynecology.
This case occurred while I was studying my last career clinic, which is precisely Gynecology and Obstetrics, and I had the opportunity to help and participate in the different areas of consultation of said service; This is how I learned about the case of Mrs. Rosa, who was sent to our office with a presumptive diagnosis of ovarian tumor; and after performing more diagnostic tests that confirmed the presence of a neoplasm, and an intensive pre-operative due to the various basic pathologies that the patient presented, the surgical approach of the patient was decided under the diagnosis of: Right Ovarian Tumor.
We see how the decision to carry out an operation on this patient, despite the many concomitant diseases that she presented, is based mainly on her age, since in patients with ovarian tumors that are within the age group greater than at 40 years old, the possibility and risk of malignancy is much higher compared to young patients; In addition to this, in the imaging studies carried out to confirm the diagnosis of neoplasia, the presence of a tumor in the right ovary, with a cystic appearance and a fairly large size (approximately 35 cm in diameter), evidenced the risk of an unfavorable evolution if more time was allowed to pass.
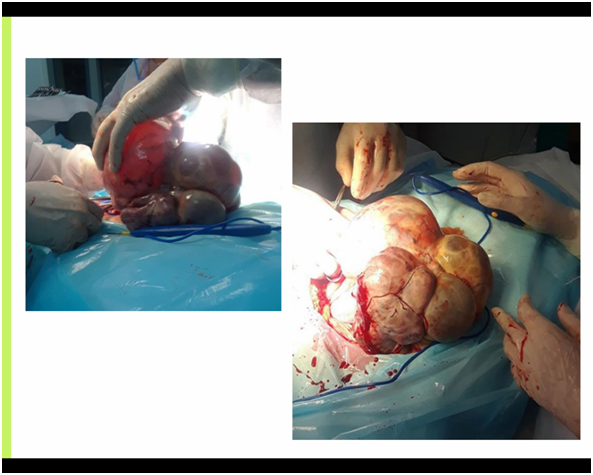
Once again I had the opportunity to be present in the surgery, which fortunately developed favorably, the patient was induced to sleep with the technique of high conductive anesthesia, and the tumor of the right ovary was removed, following the protocol of ovarian neoplasia, and a tumor of cystic appearance of 37.5 cm in diameter was obtained, and that from the point of view * macroscopic * met the characteristics of a ** Mucinous Cystadenoma **: these benign tumors of epithelial origin they are large cystic masses, multilobed from the outer capsule, and may or may not have the presence of trabeculae or partitions of fibrocollagen tissue occupied by a filament or mucoid material.

However, to confirm the type of tumor, a sample was sent to the pathology, since they will be the one responsibles for giving a definitive diagnosis based on the histological properties of the tumor.
Fortunately, the patient had an excellent evolution during the intraoperative period, so a favorable recovery is expected; and depending on the results of the pathology study, the behavior will be decided after the postoperative period.
For now, we can be satisfied with the results since during the surgical exploration there were no signs that indicate the presence of malignancy in the tumor, or of metastasis or invasion of neighboring structures; In addition to the fact that the patient was hemodynamically stable throughout the entire process, something that a patient with more than one underlying disease is essential.
CONCLUSIONS:
Ovarian tumors, like all neoplastic pathology, consist of a wide variety of presentations; they in particular can be classified according to the type of tissue that gave rise to them, in tumors of the superficial epithelium, germ cells, or stroma of the sex cords. Despite this large variety of tumors, most are characterized by being benign in nature fortunately; However, this shouldn't detract from the importance of malignant processes at the ovarian level, since despite being a minority compared to benign tumors, they still constitute about 50% of all deaths from malignant neoplasms of female genital origin.
Because in a large part of the cases, these tumors occur asymptomatically, or only with the development of an abdominal perimeter growth (as was the case of the patient that was discussed), it's very important to consider this type of pathologies in patients presenting any of the aforementioned risk factors (personal, such as nulliparity, or related to a history of this pathology in direct relatives); or in any female patient who consults for a progressive and chronic growth of the abdomen.
And since the diagnostic methods that exist little allow us the clinical differentiation between a tumor of benign nature of a malignant one, the treatment of choice is almost always the surgical removal of the tumor, for its later pathological evaluation, since this allows us to follow the behavior most appropriate to each case, always remembering the importance of the individualization of each patient.
Bibliographic references:
[1] Wiliams - Gynecology 9th Edition.
[2] Novak Gynecology - Jonathan S. Berek 14th Edition
[3] Gynecology of González - Merlo. 9th Edition.
[4] Principles of Gynecology - SEGO (Spanish Society of Gynecology and Obstetrics).
[5] Robbins - Human Pathology 9th Edition.
Best regards dear Steemit community, especially to #steemstem, who continually show their support for the medical content I share with you. I hope I have contributed to the growth of these large communities with this article.
This time I wanted to make this publication based on the high prevalence of this disease worldwide, with the intention of always providing good content and relevant information that allows us to continue nurturing our knowledge.
Until our next meeting! :)

@tipu curate
Upvoted 👌 (Mana: 15/25 - need recharge?)
Hello @iradyjr very good content thanks for this! I recommend you to leave a warning about the images of your post at the beginning or place the tag #nsfw since the images can be strong for certain people
This post has been voted on by the SteemSTEM curation team and voting trail. It is elligible for support from @curie and @minnowbooster.
If you appreciate the work we are doing, then consider supporting our witness @stem.witness. Additional witness support to the curie witness would be appreciated as well.
For additional information please join us on the SteemSTEM discord and to get to know the rest of the community!
Please consider using the steemstem.io app and/or including @steemstem in the list of beneficiaries of this post. This could yield a stronger support from SteemSTEM.